
Lumbar Puncture Procedure: Lumbar Puncture (LP) is an invasive diagnostic procedure that involves inserting a spinal needle into the lumbar subarachnoid space to withdraw cerebrospinal fluid (CSF).
- Considered a confirmatory diagnostic test for meningitis (AIIMS, RRB, DSSSB)
- First introduced in 1891 by Heinrich Quincke
- Also known as a Spinal Tap
Lumbar Puncture Procedure
A lumbar puncture, also known as a spinal tap, may be done to: Collect cerebrospinal fluid to check for infections, inflammation or other diseases. Measure the pressure of cerebrospinal fluid. Inject spinal anesthetics, chemotherapy or other medicines.
Purpose of Lumbar Puncture
- Diagnostic use: especially in meningitis, multiple sclerosis, and subarachnoid hemorrhage
- Measurement of CSF pressure
- Therapeutic purpose: relieve intracranial pressure
- Instillation of substances: medications, contrast dye, or air
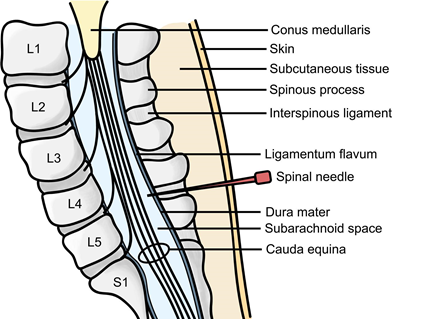
Site of Needle Insertion
- Infants & Small Children: Between L4-L5 (because the spinal cord ends at a lower level)
- Older Children & Adults: Between L3-L4 or L4-L5 (safer zones below the conus medullaris)
(JIPMER, NORCET 2023)
⚠️ Contraindications for Lumbar Puncture
- Increased Intracranial Pressure (ICP) → risk of brain herniation
- Acute spinal cord injury
- Bleeding disorders or coagulopathy
- Skin infection at puncture site
- Platelet count < 20,000 cells/mm³
- Cerebral herniation
- Previous lumbar spine surgery
- Non-communicating hydrocephalus
Required Equipment for Lumbar Puncture
- LP/Spinal needle
- Adults: 20G to 22G
- Children/Infants: 23G to 25G
- Manometer: for measuring CSF pressure
- Betadine: antiseptic for skin prep
- 3 Specimen Tubes: for bacterial, cytological, and viral analysis
- 3-Way Stopcock and Drapes
- Local anesthesia: 2% Xylocaine
Normal CSF Pressure Values
- Lying position: 5-15 mmHg OR 60-180 cm H2O
- Sitting position: 15-25 mmHg OR 200-300 cm H2O
Storage of CSF Samples
- At Room Temperature: Valid for 2-6 hours
- For Long-Term Storage: Keep at -80°C
Common Complications of Lumbar Puncture
- Post-Dural Puncture Headache (PDPH): most common; also called post-lumbar puncture headache
- Brain Herniation: if too much CSF is removed (>10 ml)
- Infection: due to poor aseptic technique
- Bleeding: especially in patients with bleeding disorders
- CSF Leakage: caused by improper dressing
- Localized Pain: manage with cold compress or ice application
- Subarachnoid Epidermoid Cyst: a long-term complication
Pre-Procedure Nursing Interventions
- Obtain informed consent
- Ensure bladder is emptied before the procedure
- Explain the procedure to reduce patient anxiety
- Prepare 3-4 sterile vials for specimen collection and label appropriately
- Use a small gauge, non-cutting, pencil-tip needle to reduce PDPH risk
- Administer 2% Xylocaine for local anesthesia
Specimen Collection Protocol
- Withdraw only 8-10 ml of CSF in total:
- Vial 1: Gram stain, culture & sensitivity
- Vial 2: Glucose and protein
- Vial 3: Cell count and differential
- Vial 4: For special tests (if needed)
- Maintain strict sterile technique throughout
- If bloody CSF appears, immediately withdraw the needle
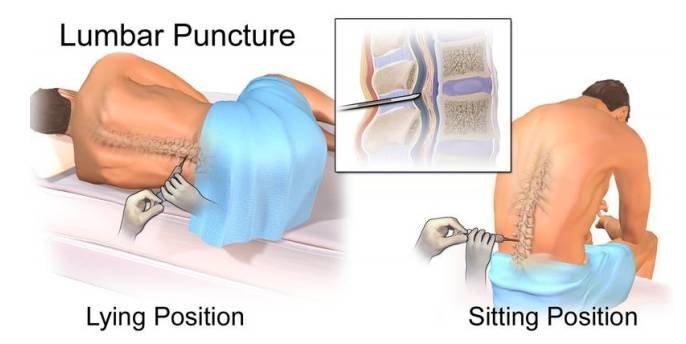
Recommended Patient Position During Lumbar Puncture Procedure
1. Left Lateral Recumbent / C-Shaped Position:
- Most commonly used
- Patient curls knees to abdomen with chin to chest (resembles fetal position)
- Ideal for measuring opening CSF pressure
2. Sitting Position:
- Patient sits with back curved, leaning forward on a table
- Feet supported
- Alternate position if lateral view is not feasible
(FAQS, NORCET-SMOINS-2023)
Post-Procedure Nursing Care: Lumbar Puncture
✅ Preventing Post-Lumbar Puncture Headache (PLPH)
- Position the patient in a supine or flat position for 2 to 3 hours immediately after the procedure.
- Avoid elevating the head for at least 6 hours to reduce the risk of developing PLPH.
(AIIMS, PGI, JIPMER-2020, KGMU-2023)
⚠️ Rationale for Flat Positioning
- Elevating the head end post-procedure may lead to a sudden drop in intracranial pressure (ICP).
- This abrupt pressure drop can result in brain herniation and irreversible neurological damage.
(JIPMER-2016)
🧠 Monitoring and Observation
- Regularly assess vital signs and neurological status.
- Persistent or worsening headache may indicate CSF leakage from the puncture site—this requires prompt attention.
🧪 Specimen Handling
- Properly label the CSF specimen and send it immediately to the lab.
- If any delay is expected, do not refrigerate the sample; instead, store it at room temperature.
💧 Hydration and Output Monitoring
- Ensure the patient receives adequate fluids.
- Keep a close check on intake and output using an I/O chart.
Key Nursing Points
- Always follow aseptic technique
- Never exceed 10 ml CSF withdrawal at one time
- Monitor for signs of complications post-procedure
- Encourage oral fluids post-procedure to reduce risk of headache
- Educate patient to lie flat for a few hours after LP to prevent PDPH
Question 1:
In a patient, lumbar puncture procedure is going on. On-duty nursing officer which position given to the patient to facilitate this procedure? (NORCET-2022)
Options:
A. Patient’s leg flexed, knees are touched on abdomen and head flexed with chin touched on chest
B. Patient’s lying on back and turning forward
C. Patient’s leg extended, knees are touched on abdomen and head in extension position
D. Patient lying in side and head turned to one side
✅ Right Answer – A
Question 2:
Which of the following is a lumbar puncture site in paediatrics? (NORCET-5 Mains 2023)
Options:
A. L₁–L₂
B. L₃–L₄
C. L₂–L₃
D. L₄–L₅
✅ Right Answer – D
📌 Must-Know Facts: Post-Dural Puncture Headache (PDPH)
✅ Most Common Complication
The most frequent complication following a lumbar puncture is Post-Dural Puncture Headache (PDPH).
❗ Primary Cause
PDPH is commonly caused by the use of a thick, dura-cutting spinal needle.
Example: 18G Quincke needle (wide bore) increases the risk due to more CSF leakage.
🛏️ Prevention Measures
Immediately after the procedure, keep the patient in a supine or flat position for 2–3 hours.
Avoid raising the head for at least 6 hours post-procedure.
💊 Management of PDPH
Start with mild analgesics.
Combination therapy like caffeine + paracetamol (PCM) is preferred.
If the headache persists, consider using an epidural blood patch as a definitive treatment.
CSF Analysis in Meningitis
| Type | CSF Appearance | Leukocyte Count | Glucose | Protein | CSF Opening Pressure |
|---|---|---|---|---|---|
| Normal CSF | Clear | < 8 cells/mm³ | 50–80 mg/dl | 15–45 mg/dl | 90–180 mmHg |
| Bacterial Meningitis | Turbid | High | Low | High | High |
| Viral Meningitis | Clear | Low | Normal | Normal | Slightly High |
| Fungal Meningitis | Clear | Low | Low | High | Normal to High |
| TB Meningitis (TBM) | Turbid | High | Low | High | High |
Normal CSF Characteristics
| Parameter | Normal Value / Description |
|---|---|
| Colour | Clear, watery, or colorless |
| pH | ~7.4 (Slightly alkaline) |
| RBC | Absent or negligible |
| CSF Lactate | 1–3 mmol/L |
| Opening Pressure | 50–200 mm H₂O |
| Protein | 15–45 mg/dl |
| Glucose | 50–80 mg/dl |
| Total Volume | 125–150 ml |
| Daily Secretion | ~720 ml/day (0.5 ml/min) |
| Production Site | Choroid Plexus of Lateral Ventricles (FAQs) |
| Absorption Site | Arachnoid Villi (AP) |
Tags
Lumbar Puncture Procedure, lumbar puncture procedure in meningitis, csf analysis in bacterial meningitis, csf interpretation in tb meningitis, normal csf values and ranges, csf glucose protein levels in meningitis, csf pressure in different types of meningitis, csf characteristics in fungal meningitis, lumbar puncture indications and contraindications, Lumbar Puncture Procedure, Purpose of Lumbar Puncture, Contraindications for Lumbar Puncture, Common Complications of Lumbar Puncture, Recommended Patient Position During Lumbar Puncture Procedure, CSF Analysis in Meningitis, Normal CSF Characteristics
post lumbar puncture headache prevention, causes of post dural puncture headache, csf production and absorption sites, normal csf composition for nursing exams, csf analysis table for nurses, lumbar puncture complications and management, csf test for meningitis diagnosis, differences in csf in bacterial vs viral meningitis, lumbar puncture nursing responsibilities, contraindications of lumbar puncture in thrombocytopenia, csf opening pressure in various meningitis types, interpretation of csf results in meningitis
Lumbar Puncture Procedure, Purpose of Lumbar Puncture, Contraindications for Lumbar Puncture, Common Complications of Lumbar Puncture, Recommended Patient Position During Lumbar Puncture Procedure, CSF Analysis in Meningitis, Normal CSF Characteristics
